
Related Posts

YOGA TO REGULATE THE AUTONOMIC NERVOUS SYSTEM
Related PostsYoga,...

IS ALCOHOL A HEALTH FOOD? ALCOHOL AND YOUR HEART
Related PostsWelcome to...

METABOLIC DYSFUNCTION AND THE ATHEROGENIC LIPID PROFILE
Related PostsWelcome to...

THIS IS YOUR HEART WITH METABOLIC DYSFUNCTION
Related PostsWelcome to...

METABOLIC HEALTH IS MORE IMPORTANT THAN WEIGHT LOSS
Related PostsWelcome to...

ARE YOU DEFICIENT IN OMEGA-3 FATTY ACIDS?
Related PostsRecently,...

WILL FISH OIL HELP OR HURT YOUR HEART?
Related PostsOmega-3...

GRAINS: HEALTH FOOD OR POISON?
Related PostsGrains are...

A TURN TOWARD NATURE TO SOLVE THE “PROBLEMS” WITH MEAT
Related PostsWhat’s up...

EARLY ABLATION FOR ATRIAL FIBRILLATION: IS IT BETTER THAN LIFESTYLE MODIFICATIONS?
Related PostsIn my...

PASS THE SALT
Related PostsSalt is in...
THE FUTURE OF PLAQUE IMAGING & DIAGNOSING CORONARY ARTERY DISEASE
Related PostsWhat is...
SHOULD YOU WEAR A CONTINUOUS GLUCOSE MONITOR?
Related Posts Many of...

FASTING SAFELY AND SUCCESSFULLY WITH DIABETES
Related Posts Almost...

THE “SAD” AMERICAN DIET
Related Posts What is...

HEART DISEASE IS DIFFERENT IN WOMEN
Related PostsThe...

THE 6 KEYS TO FASTING SAFELY WITH HEART DISEASE
Related PostsIf you...
IS YOUR GUT THE CAUSE OF YOUR HEART DISEASE?
Related PostsAt...

BENEFITS OF INCREASING YOUR MUSCLE MASS
Related PostsYou may...

ABLATION AND BEYOND FOR ATRIAL FIBRILLATION
Related PostsShould...

MYTHS & TRUTHS ABOUT WOMEN AND FASTING
Patients and people in our fasting community often ask me if fasting has a different impact on women. Many women have participated in our community fast in the last 2 years, so Beth and I have first-hand anecdotal experience that women do well with fasting. There’s a great deal of physiologic diversity among this group: young and old, physically fit and deconditioned, premenopausal and post-menopausal, metabolically healthy and diabetic, some on birth control pills, and some on hormone replacement therapy, some with longstanding weight issues, and some with changing body composition.
Fasting isn’t a practice we do in a vacuum. It’s one facet of a lifestyle that supports healthy body composition, metabolic health, and healing. The differences in physiology between men and women, and among women, will determine the effectiveness of fasting; the likelihood of side effects; and how long, how often, and how strictly to fast.
I don’t want to tell you whether women “should” fast. Instead, I want to provide information and tools so that women can personalize fasting and lifestyle changes.
Estrogen and body fat distribution
The ways our bodies store fat is a result of thousands of years of evolution, back when humans had to hunt and gather food and often fasted out of necessity.
Fat is one critical difference between women and men. It’s not just a matter of physical appearance: fat goes to different places on a woman’s body and has different functions in different places. Fat storage and utilization patterns in women prioritize sufficient energy storage for gestation and lactation. Fat storage and utilization patterns in men are a balance of quick access to energy for physical activity and of maintaining reserves for a rainy day.
Fat stored under our skin, subcutaneous adipose tissue (called SCAT for short) is predominant on the lower body—hips and thighs—of women and the upper body—chest and stomach—of men. Estrogen causes this difference in fat distribution, as well as women’s generally higher body fat percentage.
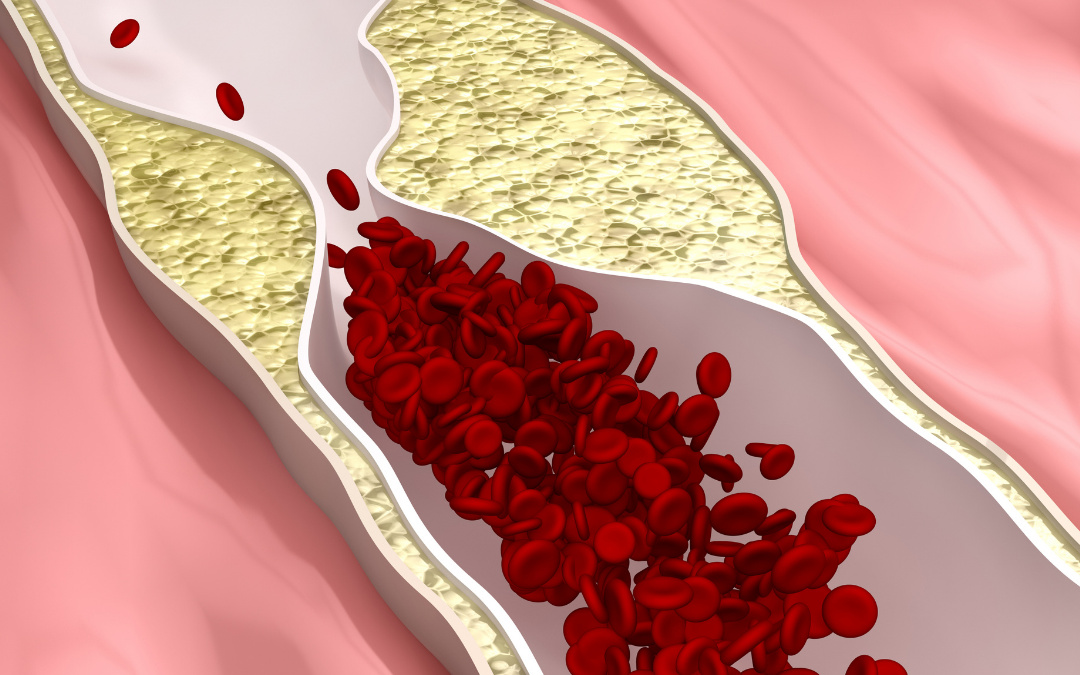
There’s another type of fat we all carry, visceral adipose tissue (VAT). Women typically carry less VAT than men do, thanks to estrogen. The SCAT caused by estrogen protects women from metabolic syndrome and heart disease, while the VAT that occurs when estrogen is lower makes you more susceptible to heart disease and metabolic syndrome.
Insulin resistance
Myth: Women should not fast because it causes insulin resistance.
Truth: This is seldom a problem. Fasting-induced insulin resistance is corrected when we break a fast and restore carbohydrate intake.
Insulin has multiple actions related to energy usage and storage. It’s the main switch that determines whether your body will store fat or mobilize it for fuel.
Insulin regulates the utilization of glucose for energy. After a meal, the glucose we’ve eaten must go somewhere quickly so that it doesn’t build up in the blood. Insulin sends about 80% of the glucose we eat to our muscles. But when the muscle is unable to respond to insulin’s signals correctly, insulin levels compensate by going up. Eventually, however, that compensation isn’t adequate and blood glucose levels go up. This is the most common form of insulin resistance, which leads to metabolic dysfunction, visceral fat, and heart disease. Women use less glucose for fuel than men and have relative insulin resistance in muscle.
Insulin is high after we eat and directs mobilization of glucose for fuel and storage of fat. Elevated insulin levels after a meal encourage fat storage. During fasting, when insulin levels are low, fatty acids (FFA) are mobilized from storage to be used as fuel. This is called lipolysis, or breaking down fat.
Some fatty acids are used for fuel, and your liver processes some into triglycerides (TG) before returning to your body’s fat stores. The fat we eat is stored directly as fat cells. But in general, your body’s insulin determines what happens to the fat in your body. It’s also affected by estrogen. Insulin resistance is different in men and women because of estrogen. Women have lower fasting glucose, and higher post-meal glucose.
Insulin determines how much glucose your liver manufactures, called gluconeogenesis. When insulin levels are lower, such as when fasting, glucose formation increases to feed the brain. Women have greater resistance to low insulin levels and they produce less glucose. This results in low fasting glucose levels and a tendency toward hypoglycemia.
The effects of estrogen
Estrogen does more than impact how a woman’s body stores fat, of course.
- Estrogen increases pancreatic insulin secretion; this may lower women’s fasting glucose level.
- Estrogen may have some effect on resting metabolic rate (RMR) in brown adipose tissue. That is, it may increase the density of mitochondria in fat to generate heat. This effect is not well documented.
- Estrogen enhances the action of leptin, a hormone that suppresses hunger in our hypothalamus. The loss of estrogen in menopause is a significant contributor to increased appetite and weight.
- Estrogen stimulates mTOR, the muscle protein synthesis pathway.
Fasting and mindful eating practices can counter the effects of reduced estrogen, such as increased appetite.
Premenopausal obesity can magnify estrogen effects, further increasing SCAT and FFA flux, and perpetuate obesity. Estrogen detoxification, in which estrogen is converted to safe forms that the body eliminates, may help along with fasting and lifestyle change to defeat this situation.
Estrogen does not completely prevent metabolic dysfunction. Genetic predisposition or dietary patterns may increase visceral fat, even in premenopausal women. Endocrine disruptors, including environmental toxins and even cosmetics, can lower estrogen and cause visceral fat accumulation.
When androgens, including progesterone or testosterone, are dominant, the male visceral fat phenotype will emerge, such as with polycystic ovary syndrome (PCOS).
Estrogen, weight loss, and fasting
Your ability and need to lose weight and your success with fasting and lifestyle changes are impacted by whether you:
- Are premenopausal, perimenopausal, or postmenopausal
- Are androgen-dominant
- Take birth control medication
- Take HRT (and your dosage and method)
- Have low body weight
- Have an eating disorder
- Are obese
- Have metabolic dysfunction
- Have stress/cortisol/sleep issues
- Have hypothyroidism
The level of estrogen in your body affects insulin sensitivity, fatty acid/FFA flux, energy utilization, body composition, muscle mass, appetite, the insulin threshold for lipolysis, and the glucose and insulin levels achieved with fasting. These factors contribute to why women respond so individually to fasting.
These factors thus also inform the length, frequency, and strictness of fasting that’s best to achieve your health goals. They also help us determine nutritional, exercise, and other lifestyle changes that will support your health and healing.
The change: waning effects of estrogen
During menopause, a gradual loss of estrogen occurs, over an average of 4 years. The median age of menopause transition is now about 50 years. This means that women can expect to live more than 1/3 of their lives in estrogen deficiency, with dramatic implications for health.
A lack of estrogen leads your body to adopt the male pattern of energy storage and utilization. A few years after transition, a woman’s risk of cardiovascular disease (CVD) approaches that of men. Inflammation, poor sleep or sleep apnea, and changes in body composition are all common symptoms of lower estrogen.
The amount of fat mass compared to men increases even more with estrogen deficiency. Men lose more muscle, ounce for ounce, with age, but women start from a lower baseline and have less muscle to safely lose. The protein requirement for new muscle growth increases with age in men and women, called anabolic resistance. When we have reduced muscle mass, the prevalence of osteoporosis goes up. Half of postmenopausal women will suffer a bone fracture.
Fasting is very beneficial for postmenopausal women, but the added challenges of increased appetite and muscle mass loss require a comprehensive lifestyle modification approach.
Energy comes and goes: Eating, fasting, and exercise
Insulin should slow or stop lipolysis (the breakdown of fat).
Myth: Any amount of insulin with halt lipolysis.
Truth: While insulin does suppress lipolysis, lipolysis can still happen with the presence of insulin. And there is a variable degree to which insulin falls with fasting from person to person.
How much fat stores go down when fasting is different for each person. It depends on how low your insulin needs to be for lipolysis and how much insulin falls when you fast. Not surprisingly, sex and estrogen are factors, since women have higher fasting insulin levels than men.
Women’s bodies turn off lipolysis more completely than men’s, particularly in more problematic VAT. So even when we’re eating and insulin is high, lipolysis in VAT provides fatty acids directly to the liver. The possibility of overloading the liver with fatty acids makes the liver tend to insulin resistance to protect itself from overaccumulation of fatty acids. Estrogen protects women from fatty liver disease!
During both feeding and fasting, women have more fatty acid flowing through their bodies (or FFA flux). Greater fat mass in women means even more fatty acid flux. A lower-fat diet when not fasting may be healthier for some women who have trouble losing weight. Diets are never one size fits all.
When fasting, everyone’s body is proficient in going into lipolysis. In general, women use fewer fatty acids for fuel. Women also have less free fatty acid oxidation during fasting than men and rely more on glucose for fuel. The excess fatty acids that women’s bodies mobilize with lipolysis but don’t use for oxidation are stored predominantly in SCAT in the lower body—hips and thighs. Estrogen reduces VAT, preserves lower extremity SCAT, and increases the need to generate glucose and ketones in the liver for fuel during fasting.
Alternate-day fasting for 6 months in obese premenopausal women with normal fasting glucose showed reduced waist circumference, improved insulin sensitivity, reduced C-reactive protein (CRP, which causes inflammation), and improved LDL and triglyceride levels.
When exercising, both men and women use glucose predominantly for fuel, but women use somewhat more fatty acid oxidation than men. You would think this would lead to more fat burning in women, but the real difference between men and women in exercise metabolism occurs after exercise stops. Post-exercise, men have a continued increased metabolic rate (RMR), but women quickly revert to a lower RMR. This effect of estrogen preserves SCAT—and, yes, can make it harder for women to lose weight.
Some women may need to increase the strictness of their fast (or how “clean” it is) or the duration of a fast to achieve lower insulin levels. But if you tend to become hypoglycemic, you may need to reduce the strictness or duration of your fast.
More myths about sex differences and fasting
Myth: Growth hormone is low in women and they will lose too much muscle mass with fasting.
Truth: Women have lower growth hormone secretion than men, but it increases with fasting just as it does in men. Pre- and postmenopausal women have documented increased muscle mass with appropriate fasting and exercise.
Myth: Women who fast will stop ovulating.
Truth: Gonadotropins and ovulation are not affected by fasting in healthy-weight women. If you are underweight, severely stressed, overtrained, or have an eating disorder, do not fast without consulting your doctor.
Myth: Women should not fast because they’ll have an excessive stress and cortisol response.
Truth: Fasting is a stress for everyone, but it’s reasonable, hormetic stress, especially if you build up the duration and strictness over time. There is no evidence that women have an inappropriately increased stress response to fasting. Everyone who fasts should give attention to stress reduction and good sleep.
Myth: Women will get gallstones if they fast.
Truth: When we fast, bile flow decreases. Gallstones are unlikely if your diet when not fasting stimulates normal gallbladder function and you don’t already have gallstones.
Myth: Fasting causes hypothyroidism.
Truth: This is mostly true. Pituitary secretion of TSH and thyroid production of T4 remains intact with fasting. What changes with fasting, as it does with other stresses, is that there is a reduction in the conversion of T4 to the active form of thyroid hormone, T3. This is a physiologic response to decreased energy availability. It’s usually asymptomatic even with preexisting subclinical hypothyroidism, but can be symptomatic if baseline thyroid function is significantly impaired. Fasting should be deferred until hypothyroidism is corrected. We don’t currently know if T3 replacement during fasting is of any benefit.
Myth: Women respond to fasting similarly.
Truth: Women respond to fasting neither similarly to men nor to each other. The tremendous variation in estrogen effects alone requires a personalized approach to fasting for women.
Myth: Low-carb diets are best for everyone.
Truth: Diets are never one size fits all, and a lower-fat diet may be more effective for some women.
Want to experience the benefits of fasting with expert advice and support? Sign up for our monthly community fasts. Details on our Events page.